{kind=link}
{kind=link}
{kind=link}
{kind=link}
Last Chapter
Next Chapter
7. A Voiced or Breathy-Voiced Glottal Adjustment During the Articulatory Closure
7.1 General Considerations
It seems probable that all natural language dialects contain simple-released-plosive phone types in which a voiced glottal adjustment is present during some portion of the period of articulatory closure. A voiced glottal adjustment could be present before the time of articulatory closure, and extend into the period of closure; or the adjustment could be brought about during the period of closure, from some pre-existing, more open adjustment.
When, as the result of a sufficiently high transglottal pressure, the voiced adjustment results in voicing (a voiced glottal action) during some appreciable portion of the closure, the resulting phone type is commonly referred to as 'voiced' and the period of closure as a 'voiced' closure. A central goal in this chapter will be to identify some of the physiological conditions under which voicing does or does not occur .
The use of a breathy-voiced glottal adjustment to produce voicing is considered in Section 7.4. In all other sections, only voiced or tightly-voiced glottal adjustments are considered.
Assuming that voicing is an aerodynamic phenomenon (as is now generally accepted), we may conclude that for any given speaker and given transglottal pressure, there is a minimal rate of air flow at which voicing can be produced. For example, LADEFOGED and McKINNEY have plotted volume velocity against subglottal pressure for a sequence of phonations of an isolated vowel spoken at various levels of loudness and fundamental frequency by one adult, male, phonetically trained speaker (LADEFOGED and McKINNEY, 1963, Fig. 3). For all phonations in which the subglottal pressure was less than 15 cm H2O, the average glottal resistance, i.e., the quotient of average subglottal pressure divided by average volume velocity, was less than 100 W (in the units used in this work). Though no subglottal pressures were used below about 8.5 cm H2O, the data given in this figure support a hypothesis that the average glottal resistance tends to be smaller for lower subglottal pressures. This hypothesis also seems compatible with an aerodynamic concept of the voicing mechanism.
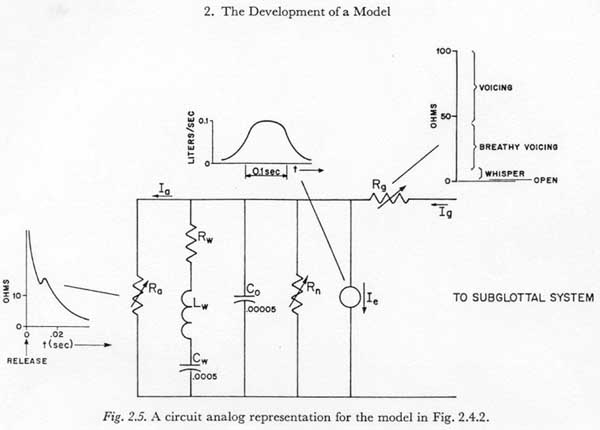
Since it is difficult to find any estimates of glottal resistance in voicing that are significantly higher than those reported by LADEFOGED and McKINNEY, let us assume that the glottal resistance in a voiced closure is equal to or less than about 80 W. From the compressibility of air, it can be computed that the compliance of a volume of air is approximately 10-3 times the volume in liters. If we assume that the supraglottal cavity volume is less than about 50 ml1, the compliance of this volume, i.e., Co in Fig. 2.5, is less than about 5 X 10-5 Farads. The time constant RgCo would then be no larger than about (80 X 5 X 10-5) sec, or 4 msec. Since 4 msec is usually less than the period of one oscillation of the true vocal folds in voicing, it can be concluded that not more than one or two such oscillations could be sustained by the air flow absorbed in compressing the air within the supraglottal cavity.
To sustain glottal oscillations with a complete articulatory closure, it is
necessary that there be another mechanism for the absorption of the glottal
air flow. The following three mechanisms may each conceivably be used for this
purpose to some degree, and will be discussed in the following sections in the
order given :
(1) a passive, pressure-actuated expansion of one or more walls of the supraglottal
cavity, i.e., Cw of Figure
2.5.
(2) a muscularly activated enlargement of the supraglottal cavity, i.e., Ie
of Figure
2.5.
(3) some nasal air flow through an incomplete velopharyngeal closure, i.e.,
through Rn of Figure
2.5.
7.2 Passive Expansion of the Supraglottal Cavity
It is obvious that certain of the walls of the supraglottal cavity, when lax, can expand appreciably in response to internal pressures. For a bilabial closure the cheeks, and the lips are the most apparent examples. Another clear example is the pushing forward of the apex of the tongue that can occur when an alveolar closure is made with the tongue tip, especially when the tongue is in the retroflex position. However, it is difficult to find quantitative estimates of the resiliency of these and other supraglottal cavity walls for the various states of tension found in speech. To obtain a rough estimate of the net compliance of the walls of the supraglottal cavity for certain places and manners of articulation, some measurements were made in the following way:
Positive and negative impulses of air flow were introduced into the supraglottal cavity by means of a hypodermic syringe (with a 5 ml total capacity) connected to the supraglottal cavity through a short length of polyethylene tubing. The resulting pressure changes were measured with a Statham strain-gage pressure transducer, type PM 283.
Alternate impulses of a fixed magnitude were generated by fixing a stop for the plunger of the hypodermic syringe so that it could move freely between its inmost position and the stop. For most of the measurements, the stop was set to limit the travel of the plunger to the one cubic centimeter mark. Some of the measurements were made with five cubic centimeters of travel. In all cases, the piston was pushed manually by the experimenter, alternately in and out with rapid strokes, at the rate of about one stroke per second (or one complete cycle every two seconds).
The resulting pressure variations were recorded on a Minneapolis Honeywell Visicorder optical recording system. The system was calibrated with a water manometer at the input to the pressure transducer .
The author served as the sole subject for the experiment. With practice it was possible to maintain a tight glottal and velopharyngeal closure fairly consistently by (1) preceding each experiment with a sizable inspiration and holding the inspired air by means of the glottal closure, (2) making the desired articulatory closure, and (3) making the velopharyngeal closure by a conscious effort to maintain a small pressure within the supraglottal cavity. The average pressure so maintained was about 5 cm H2O, though there was considerable variation within a range of about 3 to 7 cm H2O. In no case were measurements made above about 10 cm H2O.
The resulting pressure records showed alternate increases and decreases of pressure with superimposed transients and a good deal of 'noise' caused mostly by uncontrollable volume variations. About 1/3 to 1/2 of the changes in pressure level were not clearly interpretable. However, for at least half of the pressure changes, a reasonable estimation (say within about plus or minus 25 %) could be made of the change of pressure resulting from the introduction or removal of air. Measurements were made at about 1/10 to 3/10 of a second after the onset of the initial transient. By this time the transients caused by the inertance and dissipative resistance of the tissues had decayed.
The results of these experiments are summarized in Table 7.2. Measurements were made with a bilabial closure and with an alveolar closure (non-retroflex, but formed with the tongue tip).
|
Place of closure
|
Tension of walls
|
Peak to peak air volume inserted (ml)
|
Number of Measurements
|
Compliance Cw
|
|
|
Mean
|
Standard Deviation
|
||||
|
Bilabial
|
lax (including cheeks) |
5
|
13
|
0.004
|
0.00056
|
|
Bilabial
|
lax (except for tense cheeks and lips) |
1
|
8
|
0.00068
|
0.00012
|
|
Alveolar
|
lax |
1
|
7
|
0.00053
|
0.00012
|
|
Alveolar
|
tense |
1
|
8
|
0.00038
|
0.00010
|
Attempts were made to keep various structures lax or tense, as noted. For each type of cavity formation, the table shows the number of measurements of pressure change that could be made with an accuracy that was judged to be within about ± 25%. The average compliance and the corresponding variance is shown for each type.
The data in Table 7.2 can be roughly summarized by the statement that some of the more compliant walls of the supraglottal cavity, when not tensed by muscular contractions, can have a compliance of up to about 0.005 Farads: on the average, however, the compliance of the supraglottal cavity will be more nearly about 0.0005 Farads. If we use the above-mentioned value of 80 W for average glottal resistance in voicing, the time constant RgCw would be 400 msec and 40 msec respectively, for the extremely compliant and the average situations. These time constants indicate that: (1) in bilabial and retroflexed closures the walls of the supraglottal cavity can be used to absorb the glottal air flow to maintain voicing during a reasonably long articulatory closure, (2) for almost any place and manner of articulation, the walls of the supraglottal cavity can be held lax enough to absorb the glottal air flow for a period of at least 20 or 30 msec, providing there is no simultaneous compression of the supraglottal cavity due to other factors.
Just from a consideration of the range of supraglottal cavity compliance obtainable,
it appears that there are many occurrences of voiced alveolar plosives in which
the voiced interval is too long and/or the voicing too 'strong' to have been
maintained by passive supraglottal cavity expansion alone (for example, the
voiced plosives in Figure
7.4.1 and Figure
7.4.2 below). Also, there are other factors which act to negate the effect
of passive cavity expansion, and make it necessary to look for other mechanisms
which make it possible to maintain voicing. For example, there is almost always
some component of cavity volume reduction just after the time of articulatory
closure, caused by the closing motion of the articulators. (One exception might
be in a closure formed by moving the tongue forward from a highly retroflexed
position.) Also, passive supraglottal cavity expansion probably plays only a
small role in the production of voicing if the glottis is open at the time of
the articulatory closure, and if the subglottal pressure is high at that time
(as immediately following an unvoiced fricative). In this case the supraglottal
cavity pressure will be brought up to the subglottal pressure and the cavity
walls expanded before the voiced adjustment of the glottis is attained. Additional
passive expansion of the cavity walls could only be attained by reducing their
tension, but the time required for the relaxation of skeletal muscle precludes
the use of such a relaxation in most speech situations.
7.3 Active Supraglottal Cavity Enlargement
It has long been realized that the glottal air flow in a voiced plosive is often absorbed by a muscularly activated enlargement of the supraglottal cavity. Such enlargements can be thought of as being purposive, when the movements involved are not required for the production of the other features of the plosive or its neighboring phonetic units, or as non-purposive, when the volume changes result from such movements as the prerelease opening movement for the plosive or the tongue movement required for the production of the succeeding phonetic unit. The distinction between purposive and non-purposive movements may not always be clear. For example, any movements of the tongue that are made to increase the volume of the supraglottal cavity will also alter the resonances of the vocal tract during the initial portion of the succeeding phonetic unit.
To obtain an order-of-magnitude estimate of the amount of prerelease volume change associated with the opening movement of a plosive for the various places and manners of articulation, we might assume a prerelease separation of about 0.2 cm, which acts over an area of up to 15 cm2 for bilabial plosives and over as little as 5 cm2 for velar plosives. Under these conditions, this component of volume change would be between approximately one and three milliliters.
It is difficult to find a rational basis for estimating that component of supraglottal cavity volume change during the closure for a plosive which could be attributed to movements of articulation for the neighboring phonetic units. A major problem is to differentiate between a shifting of the mass of the tongue within the cavity and an outward (or inward) movement of the tongue mass. This component of volume change will not be considered quantitatively in this present work.
The important component of supraglottal cavity volume change in at least some language dialects, is the enlargement of portions of the oral and laryngeal pharynges by contractions of certain muscles of the tongue, pharynx, and neck. For example, HUDGINS and STETSON investigated the possibility of increasing the length of the pharynx in speech by the contraction of certain of the infrahyoid muscles (HUDGINS and STETSON, 1935).
Since it was difficult to find any estimates of the amount of pharyngeal expansion possible in speech, an investigation was made of the shape of the pharynx and the nature of those surrounding structures that might affect its volume. The primary references used were Grant's Atlas of Anatomy (GRANT, 1962) and Gray's Anatomy (Goss, 1959). In addition, anatomical materials were examined, and a cast was made of the pharynx of a cadaver using Geltrate elastic dental casting material2. Geltrate, in its initial liquid form, was inserted under a slight pressure into the pharyngeal cavity of an intact head of an adult male cadaver, through the esophagus. Though the shape of the cast could not be considered accurate, due to the preserved condition of the surrounding tissues, the pressure under which the liquid was inserted tended to expand those surfaces that were extensible. The resultant shape of the cast was at least roughly similar to the shape of an expanded pharynx in speech. For example, the width of the oropharynx in the anterior-posterior direction, about 1 cm, was similar to the values measured in the x-ray studies reported by PERKELL (1965).
The part of the pharynx which appears to be free to enlarge in speech without appreciably affecting the articulation of the plosive or the neighboring phonetic units is primarily the lowermost 6 cm, from the entrance to the esophagus below, to about the level of the foramen caecum of the tongue above. The upper limit would naturally be highly dependent on the place of articulation of the plosive. This lower part of the pharynx consists of a rather flat space with a lateral dimension of about 3 cm throughout its length. The upper 3 cm of this portion of the pharynx is situated behind the base (or posterior 1/3) of the tongue, while the lower 3 cm is behind the larynx. The anterior wall of the pharynx can be thought of as being composed of, or firmly attached to, the laryngeal structures and the base of the tongue. The posterior wall of the pharynx, in the section of interest, is relatively fixed medially to the spinal column through the non-distensible retropharyngeal space. Laterally, the posterior wall can be drawn inward, primarily by the inferior pharyngeal constrictor muscles below and by the middle pharyngeal constrictor muscles and the palatopharyngeus muscles above. In the upper two-thirds of the area being discussed, the posterior wall and the lateral walls of the pharyngeal space can be drawn posteriorly and laterally by the action of the stylopharyngeus muscle. This muscle originates from the base of the styloid process and enters the pharyngeal wall underneath the middle constrictor muscle, spreading out to merge with the fibers of the inner surface of the pharyngeal wall and to attach to the posterior border of the thyroid cartilage. When tensed, the stylopharyngeus muscle can be thought of as drawing the middle constrictor muscle laterally and posteriorly.
In order to estimate the range of pharyngeal volume increase possible, we will differentiate between three components of volume change, namely, the volume change caused by movements of the anterior, vertical, and posterior-lateral boundaries of the pharynx. These will be discussed in the above order .
If we consider the lateral and posterior walls of the pharynx to be held fixed, the anterior-posterior dimension of the pharynx can be increased by a forward motion of the larynx and/or base of the tongue. Forward motions of the base of the tongue of the order of magnitude of 0.5 cm have been reported by PERKELL (1965). The main activation is most likely supplied by the most inferior-posterior fibers of the genioglossus muscle to the base of the tongue, the geniohyoid muscles, and the infrahyoid muscles. The forward motion of the anterior wall of the pharynx might well be more of a pivoting around an axis somewhere near the cricoid cartilage than a uniform forward motion; however, it is difficult to find empirical evidence bearing on this question.
Another factor to be considered in the anterior expansion of the lower pharynx is the possibility that the base of the tongue does not move as a unit, but is depressed more medially than laterally. The movement of 0.5 cm measured by PERKELL was probably a maximum movement measured in the midsagittal plane. If for a movement of 0.5 cm in the midsagittal plane we can assume an average forward movement of the anterior pharyngeal wall of about 0.5 ( 2/3) = 0.33 cm, acting over the entire area of about 3 X 6 = 18 cm2, then this component of volume change could be as large as about 6.0 ml.
Though the vertical motion of the larynx-hyoid unit described by STETSON is probably partially a forward and downward tilting, the evidence appears to indicate that the vertical dimension of the pharynx can be increased up to about one centimeter by vertical movements of the larynx. For example, PERKELL has measured vertical movements of the larynx of one centimeter in x-ray studies of the production of isolated bisyllabic nonsense syllables in which the medial consonants included a number of plosives. However, in those plosives measured that were voiced, the prerelease lowering of the larynx was nowhere near the one centimeter maximum, and apparently was less than 0.2 cm.
A small vertical movement of the larynx, of the order of 0.2 to 0.4 cm, would
primarily lengthen the oral pharynx, with little effect on tongue height. Significantly
larger vertical movements would probably tend to pull down the back of the tongue
somewhat, depending on the tongue position.
Lacking further evidence, we might assume it possible to produce a vertical
elongation of the pharynx in plosive production of about 0.5 cm. If we assume
that the increase in length acts on an area slightly larger than the average
area of the oropharynx, or say about 4 cm2, then the resultilng volume
change is about 2 ml.
The third and last movement of the walls of the pharynx to be considered is the action resulting from the tension of the stylopharyngeus muscles as they pull the posterior-lateral edges of the pharynx outward (posteriorly and laterally). This is not to say that the stylopharyngeus muscles themselves must be activated; since they attach to the posterior border of the thyroid cartilage, any downward motion of the thyroid cartilage would tend to pull the stylopharyngeus muscles taut. From an examination of the structures involved, and the cast of the pharynx, it appears that each stylopharyngeus muscle might be considered to act on an area of about 2 cm2, and to move this area outward approximately 0.25 cm from a previous lax position of the pharynx. The volume change resulting from such posterior-lateral expansion would then be about 1 ml. This component of volume change might well be two or three times as large if the middle constrictor muscle, under which the stylopharyngeus passes, was previously constricted, and was relaxed simultaneously with the tensing of the stylopharyngeus. Though such coordinated opposing movements of the pharyngeal musculature are possible (and are probably common in the more extreme supraglottal cavity volume changes of an implosive), they may not be employed commonly in plosive production. However, we might add a factor of two for the possibility of some previous tenseness of the pharyngeal constrictor muscles, and conclude that a posterior-lateral expansion in plosive production can be as much as about 2.0 ml.
In summary, the forward, downward, and posterior-lateral components of a moderate expansion of the pharynx that are producible in voiced plosive production were estimated to be of the order-of-magnitude of 6.0, 2.0 and 2.0 ml, respectively. If all three actions were independently employable, the resulting maximum volume change would be as much as 10 ml. However, it is likely that one or another mechanism is favored, depending on the tongue position required for the consonant and the neighboring phonetic units. For a high tongue position, forward movements of the anterior wall are relatively easily producible. Conversely, for a low-back tongue position, vertical movements of the larynx might be more easily accommodated. For any one given context we might then expect the active pharyngeal expansion to be somewhat lower than the 10 ml obtained by summing the value computed for each component. One might estimate an expansion of from 6 to 8 ml to be attainable in most articulatory environments. Naturally, it must be kept in mind that these figures were derived from a series of rather crude approximations, and may possibly be inaccurate by a factor of two or more.
In an attempt to measure the attainable active pharyngeal volume change more directly, the author attempted to perform expansions of the pharynx in which the upper surface of the tongue was held fixed, as with the blade against the palate. The glottis was held in a tightly-voiced position so that at the end of the expansion, when voicing stopped, the glottis remained in a closed position to entrap the air drawn through the glottis. The trapped air was then expelled through a short length of tubing into a container in which the expelled air volume was measured by the method of water displacement. Volumes measured in this manner range from about 4 to 15 ml, for expansions in a range that might be called small to moderate. In interpreting these data it must be remembered that there were a great number of variables that were difficult to control, as the glottal opening, the velopharyngeal opening, and the tongue movement.
As with any other muscle-activated movement, an active expansion of the pharynx
has a minimum time constant that depends on the contractile properties of the
muscles involved and the physical properties of the structures moved. Though
it will be considered beyond the scope of this study to attempt to analyze or
estimate the dynamic properties of those structures involved in an expansion
of the pharynx, it might be hypothesized, as the result of an informal initial
investigation, that a maximal (ballistic) expansion movement would have a time
constant (as defined in Chapter 3) of about 70 to 90 msec. It might be noted
that in an active expansion of 8 ml with a time constant of 80 msec, the average
rate of transglottal air flow available is somewhat less than 8/80 = 0.1 liter/sec.
7.4 Incomplete Velopharyngeal Closure
It has long been realized that air leakage through an incomplete velopharyngeal closure may contribute toward the production of voicing during the occlusion of a plosive, at least in some language dialects (for example, MUSEHOLD, 1913, and KAISER, 1934). However, this subject has been little discussed in the recent literature, and as a result there are few data available concerning the function of the velum in such a maneuver .
In this section, a basic theoretical problem concerning the possible mechanisms for a 'nasalized' voiced plosive will first be discussed, then some evidence toward the solution of the problem will be presented. It will be argued that a significant oral pressure, as is necessary for the release of a plosive, might be difficult to maintain during a voiced closure if the mechanism for the absorption of the transglottal air flow is a velopharyngeal leakage. It appears, however, that the supraglottal pressure can be increased before the release of the closure by a breathy-voiced adjustment of the glottis, by a closing movement of the velum just before the release, or by both simultaneously.
Under the conditions of a complete oral closure, a voiced glottal adjustment and an incomplete velopharyngeal closure, the supraglottal pressure Eo is approximately
|
Eo = EsgRn/(Rn +
Rg) |
if we can neglect any changes in supraglottal cavity volume. From this relation, it follows that if the average supraglottal pressure is to build up appreciably, Rn must be of the same order of magnitude as Rg. For example, if the average supraglottal pressure is one half the subglottal pressure, then Rn would be equal to Rg. However, if the action of the glottis at that time was normal voicing, then Rg would be quite high, i.e., from 40 to 80 W. From the nature of the velopharyngeal mechanism, it is not clear whether the velum can be held in a controlled manner close enough to the pharynx to effect an air flow resistance of that magnitude. It would seem as though any air flow through the narrow orifice which would be required for a resistance of 40 to 80 W would tend to draw the velum to the pharynx and effect a closure. A small buildup in supraglottal pressure might also tend to push up the velum and close the narrow passageway.
If we assume for the sake of discussion that at normal rates of speech the mechanism for velopharyngeal closure is not consistently able to effect and hold a high air flow resistance, then we would have to look for other mechanisms by which an adequately high prerelease supraglottal pressure can be developed. Two such mechanisms occur to this author: (1) It is possible that the velopharyngeal opening could be of a transient nature, i.e., that the opening at the beginning of the period of articulatory closure could be controllably large, with a negligible average supraglottal pressure, and that the supraglottal pressure could be built up by a closing movement that is effected before the time of release. (2) Alternately, the velopharyngeal opening could be controllably large throughout the closure, and the supraglottal pressure could be built up by an increased air flow brought about by means of a transition to a breathy adjustment of the glottis.
A breathy adjustment of the glottis at or near the time of release of a voiced plosive is commonly thought to occur in the phonoaspirated3 plosives that are found, for example, in some of the languages of India. Of importance here is the observation that these same language dialects seem to contain a significant nasalization of the voiced plosives, and of the phonoaspirated plosives in particular.
In order to study further the relationships among nasalization, voicing, and aspiration in language dialects containing phono-aspirated plosives, narrow and wide band spectrograms were made of recorded samples of this sound type, and its contrasting counterparts, as spoken by native speakers of a number of Indian languages. Some of the original tapes, including those made with simultaneous recordings of supraglottal pressure, as described previously in Section 3.4, were recorded under the supervision of the author, while the other recordings were from the tape file of the Communication Sciences Laboratory or were obtained from the Language Laboratory of The University of Michigan. The recordings not made under the control of the author sounded clear and sufficiently undistorted for the qualitative observations which were to be made from them. The recordings used are listed in Table 7.4. All plosives analyzed were either in the initial position (after a breath pause) or were intervocalic.
Table 7.4
Recordings of phonoaspirated plosive
|
Speaker
|
Sex
|
Native language
|
Source
|
Material
|
| M.V. |
M
|
Hindi
|
M.R.
|
words and phrases in a list
|
| S.S. |
M
|
Hindi
|
M.R.
|
words and phrases in a list
|
| J.S. |
M
|
Hindi (Bangru Dialect)
|
Communication Sciences Laboratory
|
words and phrases in a list
|
| E.R. |
M
|
Telegu (a southern Dravidian language)
|
Communication Sciences Laboratory
|
words intermixed with commentary
|
| Not Recorded |
F
|
Hindustani
|
Language Laboratory
|
words in a list
|
The results of an analysis of the spectrographic data and pressure records
will be presented here as a series of hypotheses concerning the function of
the velum and glottis in phonoaspirated plosives of the dialects sampled:
(1) The 'aspiration' is attributable to a ballistic cyclic opening movement
of the glottis, voiced-breathy-voiced. From the discussion in Chapter 6 above,
it might be predicted that such a movement would have an average duration of
about 100 msec. This hypothesis seemed to be verified by the spectrographic
data.
(2) The initial, opening movement of the cyclic glottal gesture tends to start
20 to 40 msec before the release. The closing movement would then tend to be
completed about 60 to 80 msec after the release. The one consistent exception
to this rule was speaker J. S. who spoke the Bangru dialect of Hindi natively.
With this speaker, the breathy period seemed to be consistently initiated 20
to 50 msec after the release.
(3) In the initial position, after a breath pause, the velum is first somewhat
open and tends to close during the period of articulatory closure. Intervocalically,
between non-nasalized phonetic units, the situation is not as clear. The velum
would presumably have to make a cyclic, closed-open-closed gesture that was
approximately simultaneous with the period of articulatory closure; however,
no clear evidence for such a movement could be found. The dynamic constraints
in this type of movement of the velum may be significant to the problem.
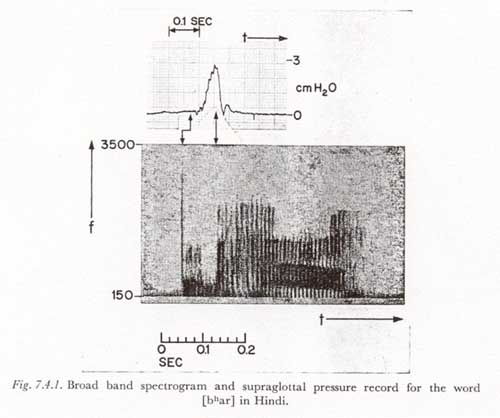
These hypotheses are illustrated in Figure 7.4.1 in which are shown a spectrogram and a record of average supraglottal pressure for the utterance [bhar], as spoken by M.V. During the initial 20 to 40 msec after the voicing starts, the average supraglottal pressure remains at approximately zero. This condition rarely occurs during a voiced articulatory closure unless the velopharyngeal pathway is not closed. In the above-indicated utterance the opening movement of the glottis appears to begin approximately at the time of the release (instead of before the release as is more typical) .This movement is evidenced by indications on the spectrogram of a weakening of the harmonic structure and an increase in the aperiodicity of the acoustic wave immediately after the release.
In the case of an intervocalic phonoaspirated plosive, one would naturally expect a cyclic ballistic gesture, voiced-breathy-voiced, and this seemed clearly the case for all records taken intervocalically. However, after an unvoiced phonetic unit such as a breath pause, there is the possibility of a unidirectional movement, open to breathy-voiced. To determine the nature of the glottal movement after a breath pause, two repetitions of the Hindi word [bhar] were produced by an adult, male native speaker of Bengali who was fluent in Hindi (not one of the subjects listed in Table 7.4), using the technique described above for bypassing the bilabial closure. As above, each repetition was in a short sequence of words and was preceded by a breath pause. The resulting records showed clearly that, at least for this speaker, the glottis was first closed for voicing, then opened in a ballistic cyclic opening movement. The total glottal movement for producing [ # bha] was open - voiced - breathy-voiced.
We have argued that a breathy adjustment might sometimes be necessary if there is to be a buildup of supraglottal pressure during the closure of a nasalized voiced plosive. The converse can also be argued, i.e., that the high air flow possible with velopharyngeal leakage (as compared with the other mechanisms discussed for the maintenance of voicing) may sometimes be required to support the oscillations of the true vocal folds when they are in the breathy-voiced position during the closure of a voiced plosive. If an air flow of more than 0.3 liter/sec were necessary to sustain oscillations of the true vocal folds with a typical breathy adjustment of the glottis, and if a maximum expansion of the supraglottal cavity (including passive and active components) for certain places of articulation may be as little as 10 ml, then the period during which voicing could be maintained without velopharyngeal leakage under these conditions would be less than 10/0.3 = 33 msec4.
The above comments concerning the relation between breathy-voice and velopharyngeal leakage may also have some relevance to dialectal and individual speech patterns within languages that do not contain a phonemically distinct set of phonoaspirated plosives. For example, it is possible that voiced plosives may tend to become nasalized in very breathy speech, especially if 'voicing' of plosives is an important phonetic feature of the dialect spoken. It is also likely that an individual having a speech pattern that is characterized by incomplete closure between the oral and nasal cavities might also tend to employ a breathy adjustment of the glottis during voiced plosives, in order to effect a buildup in supraglottal pressure.
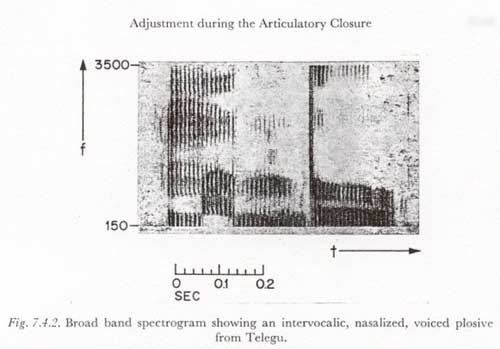
A nasalized closure of a voiced plosive can also occur without a breathy adjustment
of the glottis. For each of the informants who spoke one of the dialects containing
phonoaspirated plosives, a tendency was noted for the non-aspirated plosives
to be nasalized. An interesting example is shown in Figure
7.4.2. This figure shows a spectrogram of the word [m É
b' U], as spoken by informant E.R., the speaker
of Telegu. The prime shown with the [b] is only meant
to indicate its unusual nature, and is not used here with any special phonetic
connotation. In the spectrogram one can compare the spectrum for the closure
of the medial [b'] with the spectral structure of the
initial [m]. The spectra for the two sounds are similar
except that the higher frequencies are much less predominant in the closure
of the [b']. It is a reasonable hypothesis that in this
utterance the velopharyngeal passageway was kept open during most or all of
the closure of the plosive, but at an opening considerably less than that normally
used by this speaker for the nasal. Two other observations that can be made
are as follows:
(1) The unusually long closure and the constancy of the character of the spectrum
over a large portion of the closure indicated that the hypothesized partially
open position of the velopharyngeal passageway was not entirely a transient
or transitional phenomenon. The possibility of a phonetically significant steady-state
adjustment of the velum between 'open' and 'closed' is of some theoretical interest
in physiological phonetics.
(2) The presence of strong, harmonic-rich voicing immediately after the release
indicates that the glottis was in a voiced adjustment just before the release.
(In fact, the presence of relatively strong harmonics at frequencies over 3000
Hz, in the region of the fourth formant, indicates to this author that the glottis
may have been adjusted somewhat tighter at the time of release than would be
common for the speaker during a common 'voiced' adjustment.) The strong explosion
indicates that there was a significantly high supraglottal pressure before the
release. It is likely that this pressure was produced or augmented by a transition
from an intermediately open velopharyngeal passageway to a fully closed passageway
during the latter part of the articulatory closure, as discussed above.
The experimental observations presented above concerning the function of the
velum in the voiced plosives of certain languages should be considered exploratory
rather than conclusive in nature. It appears that a great deal would be gained
in our knowledge of the functioning of the velum in speech from a much more
detailed quantitative study of the voiced plosives of the various Indian languages.
It should be especially valuable to simultaneously record the air flow from
the nose (or the nose and mouth together), the supraglottal pressure, and the
radiated acoustic wave. Simultaneous x-ray measurements of the action of the
velum would also be highly informative.
7.5 Variations in Subglottal Pressure
In this section a complete velopharyngeal closure will always be assumed. It
is shown in Section 7.2 above that during the period of articulatory closure
the compliance of the walls of the supraglottal cavity (Cw) is often
large enough to absorb the transglottal air flow necessary for voicing for an
appreciable period of time. There are two common situations in which a large
compliance Cw can be effective in the production of voicing:
(1) A subglottal pressure is present before the articulatory closure and remains
essentially constant during the period of closure, providing the glottis is
in a voiced adjustment (or an adjustment more closed than a voiced adjustment)
at the time of the articulatory closing gesture.
(2) During the period of articulatory closure the glottis is in a voiced adjustment
and the subglottal pressure is increasing.
The first condition occurs commonly in an intervocalic voiced plosive. If there were no appreciable active supraglottal cavity volume change, the result ,would be (ideally) an exponentially decaying transglottal air flow (and therefore a similarly decaying radiated acoustic signal), as Cw is 'charged' to subglottal pressure.
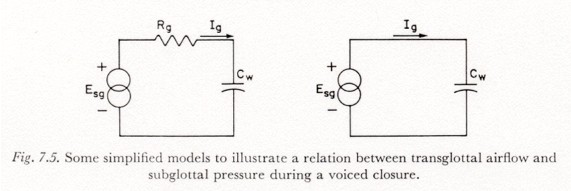
The second condition occurs commonly in a voiced plosive directly following a breath pause, if the subglottal pressure increase following the pause takes place during the period of articulatory closure. The relation between transglottal air flow and the variation in subglottal pressure will be derived at this point, under the assumptions: (1) that when the voiced glottal adjustment is attained there is not a large difference between subglottal and supraglottal pressure (this essentially means that there was no previous retention of subglottal air by a tight glottal closure); (2) that there is not an appreciable active change in supraglottal cavity volume; (3) that the average glottal resistance Rg is less than 75 W; (4) that Cw is less than 0.001 (Section 7.2 ; this assumption would not hold for a bilabial closure with lax cheeks or lips); (5) that the minimum time constant of the increase in subglottal pressure Esg is 150 msec (Chapter 3); and (6) that the inertive and resistive supraglottal wall parameters Lw and Rw can be neglected for a subglottal pressure variation time constant of over 150 msec. As noted above, a complete velopharyngeal closure is assumed. Figure 7.5A shows the relationship between the parameters Esg, Rg, and Cw under these assumptions. Co is negligible and is not represented.
The time constant RgCw is less than 75 X 0.001 = 0.075 sec. Since the time constant of the source Esg is assumed longer than 0.15 sec, we can assume that under most conditions the time constant RgCw can be considered small and Rg can be initially neglected. This is especially true for alveolar and velar places of articulation, in which Cw tends to be smaller than the maximum assumed. The resulting model is represented in Figure 7.5B. The desired relationship between the parameters of Figure 7.5B is simply:
Ig = Cw dEsg/dt.
This expression says that the transglottal air flow will vary as the slope (rate of change) of the supraglottal pressure increase. To see the order of magnitude of Ig, let us assume rather high values for both dEsg/dt and Cw, say 80 cm H2O/sec for dEsg/dt (as would be produced by an asymptotic increase of 12 cm H2O with a time constant of 150 msec) and 0.001 for Cw (Table 7.2). Under these conditions Ig is 80 X 0.001 = 0.08 liter/sec. If we consider that a transglottal air flow rate of between 0.05 and 0.1 liter/sec is probably required to sustain a steady-state voicing under most voiced adjustments of the glottis, it can be seen that this component of transglottal air flow (due to an increase of subglottal pressure acting on Cw) may often be minimally able to support voicing, or at least be a critical factor in determining the occurrence or non-occurrence of voicing.
The above observations may be of significance in explaining the variability in the occurrence of voicing when a 'voiced plosive' phoneme occurs immediately after a breath pause in some language dialects. If we could assume that the component of air flow discussed above is the primary mechanism for producing transglottal air flow, there would be two cases of interest :
(1) If the voiced glottal adjustment occurred early in the period of closure, the occurrence of voicing would depend heavily on the rate of increase of subglottal pressure, on Cw, on the exact adjustment of the glottis within the set of voiced adjustments, and on the presence of other simultaneous contributions to transglottal air flow (such as the increase in supraglottal cavity volume due to the articulatory opening gesture). Some voicing would usually occur, and when voicing occurs, the amplitude of the oscillation of the true vocal folds, and therefore of the radiated acoustic signal, would tend to be modulated in proportion to the slope of Esg.
(2) If the voiced glottal adjustment occurred late in the period of articulatory closure (as is apparently common in some dialects of English), the occurrence of voicing would depend on the factors mentioned above, and in addition on the timing of the articulatory and respiratory movements. Voicing would most likely occur when the increase in subglottal pressure is timed so that the period of its maximum derivative occurs just before the time of the articulatory release (i.e., simultaneous with the short period of voiced glottal adjustment before the release).
An important question is raised concerning prevocalic plosives that immediately
follow a breath pause and that have a voiced glottal adjustment which is attained
during or before the period of articulatory closure (and not after the release).
If the voiced glottal adjustment is not accompanied by a significantly active
increase in supraglottal cavity volume or by incomplete velopharyngeal closure,
then the occurrence or non-occurrence of voicing is strongly dependent on a
number of factors not normally considered to be purposively controlled for the
production of phonetic distinctions. This is especially true if the voiced adjustment
is attained late in the period of articulatory closure. An important theoretical
question is whether the phonetic description of such a plosive production might
not more meaningfully refer to the presence of the voiced glottal adjustment
during the articulatory closure, rather than to the occurrence or non-occurrence
of an oscillation of the true vocal folds that is sufficiently strong to be
called 'voicing'.
Last Chapter |
Next Chapter |